Part I: Review of Special Population
Chosen Group
The chosen population for this comprehensive wellness program is the elderly members of the community. Working with the elderly members of the community is a fulfilling aspect of nursing practice, especially due to the fact that they need attention, time, and utmost care. Different research studies have been conducted to understand various aspects of care provision for the elderly depending on different diseases. This comprehensive wellness program will focus on problems associated with the elderly, including incontinence, sleep problem, delirium, evidence of falls, confusion, pressure ulcers, feeding problems, dizziness, and frailty. Additionally, it will focus on nutrition, skin breakdown, hearing, pain, elder abuse, alcohol use, and fatigue. Different healthcare providers focus on specific aspects of care for the elderly populations depending on their scope of practice. Therefore, some researchers have dedicated their studies to function or independence through tools such as the daily living scores. The wellness program will focus on most of these phenomena relating to the elderly members of society.
The aging population in the United States and globally has been significantly increasing as well as their healthcare needs. Estimates from the World Health Organization (WHO) suggest that the proportion of the world’s population above 60 years will nearly double from 12 percent to 22 percent between 2015 and 2050 (Olshansky & Carnes, 2010). The increasing number of the aging population would be associated with significant challenges to the health and social systems of the countries significantly affected by the demographic shift in age. In 2016, the population aged above 65 years was about 15.2 percent, representing 49.2 million Americans, or about 1 in every seven Americans (Administration for Community Living, 2018). This represents an increase from 37.2 million within the previous ten years in 2006 and is projected to reach 98 million in 2060 (Administration for Community Living, 2018). The population aged over 85 years is also expected to increase by about 129 percent between 2016 and 2040 from 6.4 million to 14.6 million (Administration for Community Living, 2018).
The increase in the number of the aging population has been attributed to different factors. While in some research studies, increasing longevity and declining fertility have been associated with the demographic shift, other studies have considered international migration a significant driver in the population age structure in some regions and countries. According to the Department of Economic and Social Affairs of eh United Nations Secretariat, the demographic transition in Europe and the United States driven by reductions in fertility and improvements in survival by the late nineteenth century is the reason they have some of the world’s most aged population (United Nations, 2019). A snapshot of the fast-growing United States older population also associated the increase in the number of the elderly population to increased birth rates and longevity (Roberts et al., 2018). Migrations have also contributed to the rise in the aging population in the United States because most immigrants are of working ages, which alters the age structure of the recipient countries (United Nations, 2019). The changes in the population age structure determine the health concerns of the elderly population and its impact on the country’s healthcare provision.
Literature Review
The comprehensive wellness program will focus on the healthcare concerns of the elderly population. Different research studies have investigated the impact of aging on heal status and established that health and wellness deteriorate with age and is often associated with several comorbid chronic illnesses. Urinary incontinence (UI) has been considered a consequence of the aging process and geriatric syndrome. In a cross-sectional study of 322 diabetic patients aged 60 to 96 years and admitted to the National Geriatric Hospital, the prevalence of UI among the diabetic population of the survey was 62 percent (VU, 2018). Another study established that the limited professional competence and knowledge about urinary incontinence further complicated the provision of care for the elderly (Tomasi et al., 2017). In both cases, the researchers established that advanced age, cognitive impairment, comorbidities increased the risk of urinary incontinence in elderly patients and complicated their self-care and care by providers, including family members and other caregivers.
Other health complications associated with the aging process include sleep problem, delirium, evidence of falls, confusion, pressure ulcers, feeding problems, dizziness, nutrition, skin breakdown, hearing, pain, elder abuse, alcohol use, fatigue, and frailty. Due to incontinence, nocturia increases the risk of poor sleep quality among the population under study, especially in Asian American patients with comorbid hypertension, diabetes, and hyperlipidemia (Chiang et al., 2018). Mental health is another concern of the aging process, as is evidenced by increased delirium and confusion. Most of the patients admitted with delirium in the United States are usually 65 years or older (Reddy et al., 2017). With an increased number of comorbid conditions, the elderly population have a higher risk of having severe disturbances in their mental abilities resulting in reduced awareness of their environments and confused thinking. Consequently, they might forget basic things, including simple instruction, taking their prescriptions, heading to or returning home from their local stores, and the names of their family members.
Feeding problems, nutrition, and elder abuse are other common problems associated with the aging process. Feeding problems and nutrition could be attributed to their socioeconomic status. Most elderly populations, especially women above 75 years, are not married and out of employment and get their support from family members, social security, income from assets, private pensions, and government employee pensions (Administration for Community Living, 2018). People with lower income levels have always been associated with poor nutrition and feeding problems (Ravel et al., 2020). Elder abuse and neglect is another consequence of aging that has a severe impact on the population. Some of the risk factors associated with elder abuse and neglect include problems with physical health, mental health, substance abuse, dependency, stress and coping problems, the attitude of the caregivers and the client, relationship problems, and victimization (Storey, 2020). Some of the common consequences of elder abuse and neglect include physical injuries, disturbed sleep, malnutrition, dehydration, increased susceptibility to new illnesses, poor hygiene, and persistent pain.
Lifestyle Factors
Lifestyle factors determine the quality of lifestyle for the aging population. While positive lifestyle factors improve the quality of life during the aging process, poor lifestyle habits compromise the quality of life at a later age. Some of the positive lifestyle factors that promote successful aging include positive attitudes and state of mind, functional relationships with close friends and family members, proper nutrition, good exercise habits, meaningful activities, healthy habits, and quality of sleep. Making great choices inform how you might live your life in the elderly stages. Taking charge of your attitudes, eliminating negative self-talk, embracing a sense of humor, hope, and confidence, and having optimism have been linked to healthier and happier adult lives (Atallah et al., 2018). The need for relationships have been considered to include protecting emotional well-being, being involved in activities to help forget your woes, contact others, and maintaining meaningful relationships prolongs healthier lives.
Meaningful activities include taking and committing to activities that the client considers enjoyable, setting SMART goals, and asking yourself the things that makes you happy and keeps you going. Proper nutritional habits, good hydration, and maintaining diets high in volumes of grain, fruit, nuts, fiber, and veggies helps in maintaining body weight, thereby reducing the risk of developing heart-related diseases and other consequences of poor nutrition (Suryadinata et al., 2020). Elderly individuals also need to exercise regularly and consistently according to their health and wellness coach’s advice, including weight resistant training, stretching, balance routines, and aerobics. Physical activity and exercise keep joints working better to reduce falls, combats anxiety, and reduces the possibility of developing illnesses such as cancer (Atallah et al., 2018). Finally, getting the recommended amount and quality of sleep and seeking help if sleep problems are encountered improves the quality of life and activates mental activity.
The lifestyle factors that have been suggested to improve the quality of life in the elderly population are the same that could hinder healthy living if not carefully observed. Some of the negative lifestyle choices for the elderly include having poor diet choices, being overweight or underweight, physical inactivity, smoking, and alcohol and illicit drug use. While aging is an unavoidable natural phenomenon, biological, social lifestyles, and psychological diversity and conditions determine the rate of aging (Samarakoon et al., 2011). Research findings from a survey study established that premature aging is typical among married women with a secondary level of education and engaged in occupations that dominate physical labor (Samarakoon et al., 2011). While physical activity is encouraged, excessive physical activity increases the chances of premature aging as muscle mass and strength declines with age. Poor health choices, including smoking, drinking, irresponsible sexual activity, and illicit drug use, have also increased aging problems and developing comorbid illnesses.
Programs
Kegel Exercises for Elderly Patients with Incontinence
Incontinence is a common problem with the elderly that affects self-care and caregivers’ involvement in taking care of the elderly populations. The Kegel exercise has been used in different cases to prevent and control urinary incontinence and other pelvic floor problems in the elderly. The exercise aims to strengthen the pelvic floor muscle that supports the bladder, uterus, rectum, and small intestines. Several factors that have been associated with weakening the pelvic floor muscles, including pregnancy and childbirth in women, excessive strain from coughing or constipation, surgery, and being overweight, are some of the consequences of the aging process. Additionally, aging has been independently identified as a factor that weakens the pelvic floor (Swenson et al., 2020). The Kegel exercise is designed to help the elderly deal with weakened pelvic floor that causes incontinence.
The Kegel exercise is recommended among the elderly populations that experience symptoms, including leaking a few drops of urine while laughing, coughing, sneezing, leaking stool, or having a strong, sudden urge to urinate just before losing a large amount of urine (Saraçoğlu et al., 2018). The above types of incontinence are referred to as stress incontinence, fecal incontinence, and urinary urge incontinence, respectively. However, the Kegel exercise could also be recommended for other patients than the elderly, such as women during pregnancy or after childbirth, to help improve their symptoms. Nevertheless, the exercise is not recommended for patients with overflow incontinence or leaking small amounts of urine due to a full bladder or people who leak large amounts of urine when sneezing, laughing, or coughing. For the latter category, pharmacological treatment of the condition might be appropriate.
The Kegel exercise can be performed in different stages to help the patient. First, the patient should identify the right pelvic muscle by stopping urination midstream. The patient should then be guided on the position to do the exercise. The next thing is to get the perfect technique. The client should imagine sitting on a marble and tightening the pelvic muscles as if trying to lift the marble. The client also needs to maintain their focus on tightening the pelvic floor muscles and avoid flexing the muscles in the thighs, abdomen, or buttocks, and avoiding holding of breath. Finally, it is important to keep the correct repetitions and sets as directed by the provider to realize the benefits within a few weeks to a few months of beginning the exercise, depending on the severity of the patient’s severity and age.
Part II: Apply Skills
Counselling Techniques
Developing a therapeutic alliance with the patient is critical to the success of the selected treatment options. The diversity in counselling techniques, counsellors’ philosophies and theories of approach to treatment, and patient needs have led to the various counselling models. Some counsellors prefer to use solution-faced therapy, others subscribe to cognitive therapy, holistic health, strength-based, or person-centred approaches. Nevertheless, these counselling techniques and philosophies contend in the role of the proper therapeutic alliance between the provider and the client in the delivery of effective care. According to Carl Rogers, factors necessary for achieving constructive personality change through therapy, the client-therapist relationship is crucial to the entire process (Moore et al., 2020). He listed six factors, four of which addressed this relationship.
The four factors that Rogers addressed in his article in the Journal of Consulting Psychology emphasized that client-therapist relationship should be established to provide an enabling environment in the counselling process. He indicated that the therapist should be genuinely engaged in the therapeutic relationship, positively regard the client unconditionally, empathize with the client, and clearly communicate these attitudes (Miller & Moyers, 2017). According to these factors, it is evident that a strong therapeutic alliance strongly correlates to strong treatment outcomes than any therapeutic interventions selected for the client.
Working with the elderly in counselling requires strong therapeutic alliances. Therefore, making personal contact with the client determines the type of alliance with the therapist. First, it would be important to understand the client’s cultural and religious values and beliefs before making contact. Secondly, the therapist must understand some of the reasons that might cause clients to feel uneasy during therapy, thereby hindering the alliance. Some of these factors include a history of bad therapy, reluctance to seek treatment, the client’s mental health diagnosis, therapist’s anxiety, experience, and body language, trauma, poor choice of the therapeutic environment, and the client’s cultural and religious norms (Paap et al., 2021). Therefore, the provider must eliminate these barriers to have the best environment for the therapy.
Using the person-centred approach is the best way to make personal contact with the patient to build a good therapeutic alliance. Eliminating these barriers using the person-centred approach to therapy would require helping the client feel more welcome by creating an enabling environment. It is also important to understand that it takes time to build close and trusting therapeutic alliances. Therefore, the first few sessions may be built on small talk, surface-oriented, and occasional disclosure. Getting the client to open up requires a slow but steady build-up approach. Non-judgmental interactions with the client also build trust. Some clients might pick up the slightest hint of judgement in your comments or attitude. For instance, when working with the elderly, avoid giving medical or religious advice. Other strengths that the counsellor needs in building a therapeutic alliance include managing emotions, avoiding repeating a single question numerous times, talking about what the client wants to achieve from the therapy, planning questions ahead of time, and referring the client to another therapist if you feel ill-equipped to help the client.
Health History
The following are some of the questions I would ask the client during the initial health history assessment of an elderly client with comorbid chronic illnesses and incontinence, sleep problem, delirium, evidence of falls, confusion, pressure ulcers, feeding problems, dizziness, and frailty.
- Did you get help from others in performing activities in the past week, including getting dressed, eating, bathing, grooming, using the toilet, or walking?
- Have you been receiving help from others in taking care of things, including banking, housekeeping, using the telephone, food preparation, shopping, taking your medications, or transportation?
- In the past year, how many times have you had four or more drinks in a day?
- Have you felt anxious, nervous, or on edge over the past two weeks?
- How often were you not able to stop worrying over the past two weeks?
- Have you felt depressed, down, little pressure or interest in doing things, or hopeless in the past two weeks?
- How would you generally say your health is?
- How would you describe the condition of your mouth and teeth?
- Do you have trouble taking medication according to the doctor’s prescription?
- Over the past week, hominy times did you eat fast food, fruits or vegetable, sodas, and sweetened drinks?
- Have you felt any kinds of pain (joint pain, back pain, or muscle pain) in the last week?
- Do you engage in any physical activity, including walking, and how much time do you take with the activity?
- Do you snore when you sleep?
- Do you sleep during the day?
- Do you have trouble falling or staying asleep?
- Do you use tobacco or illicit drugs?
Elderly patients require evaluation of functional performance for planning support needed in their age. Some changes related to acute illnesses, normal aging, hospitalization, and worsening chronic illnesses can reduce the ability to perform tasks necessary for independent living. Before approving the patient for self-care, they may require clearance from a medical doctor, especially since chronic illnesses might require specific living conditions and support from community programs.
Exercise
The initial assessment that would be completed for the elderly with incontinence and other comorbid chronic illness registering for the Kegel exercise would include physical, environmental, social, and spiritual dimensions of their wellbeing. The Body-Mind-Spirit Wellness Behavior and Characteristic Inventory would be instrumental in developing the clients’ vulnerability because it entails a holistic assessment of the patient and determines the levels of vulnerability in different aspects of their life. The assessment would also consider the nutritional needs of the client.
The risk factors involved with the elderly include a reduced lower extremity strength, poor balance, changes in gait, and a history of falls, which generally increases the risks of falling during exercises. Some of the safety tips for the elderly while exercising include avoiding overdoing exercises, wearing the appropriate gear, staying hydrated, warming up properly before exercise, and being aware of their surroundings to avoid accidents. Additionally, when exercising with the elderly, following instructions and avoiding modifications of the exercises reduces the risks of accidents and strains.
Cardiovascular Endurance Exercise
One primary factor that affects cardiovascular endurance is age. During the aging process, cardiovascular endurance reduces. Additionally, body fat affects an individual’s cardiovascular endurance. Due to reduced physical activity in elderly populations, both age and increased body fat are risk factors. The selected cardiovascular exercise selected for the elderly is swimming, which requires energy to power the involved muscles produced through adenosine triphosphate (ATP). Swimming has been attributed to improved self-esteem and a positive body image, which encourages healthy living (Diaz & Diaz, 2021).
| Deliverable | Assessment | Objective | Duration |
| Body Image | Bad | Improve | 6 Weeks |
| Weight | Obese | Reduce to recommended BMI | 8 weeks |
| Body Fat Mass | Above average | Target lean | 6 weeks |
| Heart Rate | Fast | Normalize | 4 weeks |
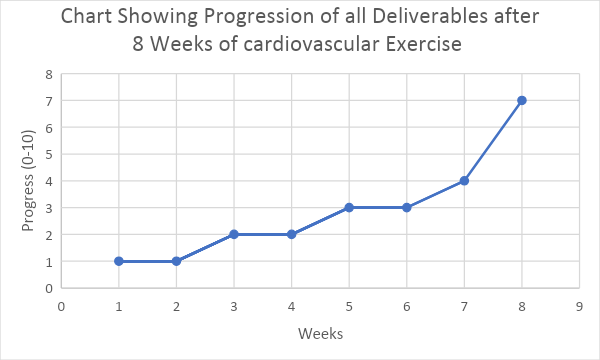
Motivational Strategies and Evaluating Progress
The two motivational strategies that would be appropriate when working on the health and wellness of the elderly population include setting action steps towards their goals and creating checkpoints. For example, introducing the elderly to a new diet and fitness plan requires setting measurable and specific goals and taking action to get there. In addition, taking pictures or monitoring glucose levels is a significant way of improving health and weight and insulin sensitivity, respectively. Creating periodic checkpoints in the wellness program is another motivational strategy that could effectively weigh into the program.
This could be done weekly or monthly encourages a sense of internal competitiveness without focusing on small details and gives the client time to notice measurable results (Bart et al., 2018). For instance, evaluating a client trying to lose weight, improving their physique, and manage their fat intake would include testing their ability in a few basic exercises, weighing themselves after a few weeks, and reviewing their diet patterns over the same period. Changes noted in these reviews would be used to set goals for the next weeks in the wellness program and adjust the objectives based on the achievements of the previous weeks.
Stress Management
The aging process comes with a lot of stress. According to clinical studies, the brain can slowly lose its skills at regulating hormone levels as the client grows old. Consequently, elderly clients who feel anxious or worried tend to produce higher amounts of stress hormones (Kumar et al., 2020). Therefore, measuring their stress levels is necessary when dealing with any health conditions. The Perceived Stress Scale (PSS) is the most widely used measurement tool for perception stress as it measures the degree to which situations in the client’s life are appraised as stressful (Kumar et al., 2020). To use the scale, the provider would require permission from the American Association Sociological Association and a PSS printed questionnaire from the author, S Cohen.
Assuming that the elderly clients require stress management, the preferred stress management techniques would be mindfulness mediation and counselling. Mindfulness meditation effectively trains clients to slow down racing thoughts, calm the mind and body, and let go of negativity. The technique involves creating the intention to cultivate awareness, paying attention to the events occurring in the present moment, and having a non-judgmental attitude. Counselling would be effective when helping the client to recognize and release stress. When the client requires to be alone, meditation would be effective over counselling and vice versa.
Dietary Guidelines
Dietary patterns could be assessed using data-driven or hypothesis-driven analysis. Additionally, assessing the nutritional status of the elderly could entail body composition estimation, anthropometric measurements, and questionnaires, including MST, MNA, PINI, and NRI. Therefore, I would recommend simultaneous use of data-driven and hypothesis-driven approaches to measure the whole grain, total vegetable, total fruit, and whole fruit intake of the elderly for the selected patient population. The dietary guidelines that I would suggest for the elderly would be nutrient-rich foods, including fruits and vegetables, low- or no-fat dairy, legumes, and high-protein foods such as lean poultry and meat, lentils, nuts, and nuts soy products. However, they should limit foods high in sugar, saturated fat, and sodium. Additionally, for physically active males aged about 70 years, 2,000-2,600 calories a day is required 1,600-2,000 calories daily is required for females with similar demographics.
Cultural Competence
Cultural competence comprises the significant steps necessary for developing a therapeutic alliance. For elderly clients with different cultural backgrounds than the provider, the latter should consider and consider the client’s values and beliefs. In most cases, when cultural differences are involved, the language barrier might hinder the development of a proper therapeutic alliance. Therefore, hiring a translator would be an effective way of promoting cultural diversity. Other activities include having providers serve clients of the same sex, having more than one provider in the room with the client of the opposite sex, having a non-judgmental attitude toward the client based on their values, sexual orientation, gender, and other sociodemographic attributes. Racial prejudice and other barriers to therapeutic alliances should be avoided during the assessment to allow the client to open up and speak freely.
Psychological Considerations
Some of the common psychological issues associated with the elderly include depression, anxiety, delirium, personality disorders, dementia, and substance abuse. Additionally, they suffer from emotional problems, including grief, autonomy, financial constraints, loneliness and lack of social networks. Therefore, the two psychological principles that may help the elderly deal with the consequences of the aging process are social interaction and competition and motivation and engagement. While social interaction and competition address cooperation and the impact of social pressure in modifying behavior, motivation and engagement help them answer the question “why do I have to complete the wellness program?” in a way that clearly illustrates the value and need for the program in a self-assessed manner.
References:
Administration for Community Living, A. on A. (2018). A profile of older Americans. In The Florida nurse (Vol. 34, Issue 4).
Atallah, N., Adjibade, M., Lelong, H., Hercberg, S., Galan, P., Assmann, K. E., & Kesse-Guyot, E. (2018). How healthy lifestyle factors at midlife relate to healthy aging. Nutrients, 10(7). https://doi.org/10.3390/nu10070854
Bart, R., Ishak, W. W., Ganjian, S., Jaffer, K. Y., Abdelmesseh, M., Hanna, S., Gohar, Y., Azar, G., Vanle, B., Dang, J., & Danovitch, I. (2018). The assessment and measurement of wellness in the clinical medical setting: A systematic review. In Innovations in Clinical Neuroscience (Vol. 15, Issues 9–10, pp. 14–23). Matrix Medical Communications. /pmc/articles/PMC6292717/
Chiang, G. S. H., Sim, B. L. H., Lee, J. J. M., & Quah, J. H. M. (2018). Determinants of poor sleep quality in elderly patients with diabetes mellitus, hyperlipidemia and hypertension in Singapore. Primary Health Care Research and Development, 19(6), 610–615. https://doi.org/10.1017/S146342361800018X
Diaz, H. P., & Diaz, E. F. (2021). Special Swimming Activity, a Recommend Program for Persons with Disabilities (PWD). J Adv Sport Phys Edu, 4(3), 30–44. https://doi.org/10.36348/jaspe.2021.v04i03.003
Kumar, R., Seangpraw, K., Auttama, N., Somrongthong, R., Tonchoy, P., & Panta, P. (2020). Stress and associated risk factors among the elderly: A cross-sectional study from rural area of Thailand. F1000Research, 8. https://doi.org/10.12688/f1000research.17903.2
Miller, W. R., & Moyers, T. B. (2017). Motivational interviewing and the clinical science of carl rogers. Journal of Consulting and Clinical Psychology, 85(8), 757–766. https://doi.org/10.1037/ccp0000179
Moore, A. J., Holden, M. A., Foster, N. E., & Jinks, C. (2020). Therapeutic alliance facilitates adherence to physiotherapy-led exercise and physical activity for older adults with knee pain: a longitudinal qualitative study. Journal of Physiotherapy, 66(1), 45–53. https://doi.org/10.1016/j.jphys.2019.11.004
Olshansky, S. J., & Carnes, B. A. (2010). Ageing and health. The Lancet. https://doi.org/10.1016/S0140-6736(09)62177-2
Paap, D., Krops, L. A., Schiphorst Preuper, H. R., Geertzen, J. H. B., Dijkstra, P. U., & Pool, G. (2021). Participants’ unspoken thoughts and feelings negatively influence the therapeutic alliance; a qualitative study in a multidisciplinary pain rehabilitation setting. Disability and Rehabilitation, 1–11. https://doi.org/10.1080/09638288.2021.1924297
Ravel, A., Mircher, C., Rebillat, A. S., Cieuta-Walti, C., & Megarbane, A. (2020). Feeding problems and gastrointestinal diseases in Down syndrome. In Archives de Pediatrie (Vol. 27, Issue 1, pp. 53–60). Elsevier Masson SAS. https://doi.org/10.1016/j.arcped.2019.11.008
Reddy, S., Irkal, J., & Srinivasamurthy, A. (2017). Postoperative delirium in elderly citizens and current practice. In Journal of Anaesthesiology Clinical Pharmacology (Vol. 33, Issue 3, pp. 291–299). Medknow Publications. https://doi.org/10.4103/joacp.JOACP_180_16
Roberts, A., Ogunwole, S., Blakeslee, L., & Rabe, M. (2018). A Snapshot of the Fast-Growing U.S. Older Population. United States Census Bureau. https://www.census.gov/library/stories/2018/10/snapshot-fast-growing-us-older-population.html
Samarakoon, S. M. S., Ravishankar, B., & Chandola, H. (2011). Effect of dietary, social, and lifestyle determinants of accelerated aging and its common clinical presentation: A survey study. AYU (An International Quarterly Journal of Research in Ayurveda), 32(3), 315. https://doi.org/10.4103/0974-8520.93906
Saraçoğlu, M., Eroğlu, A., & Divrik, R. T. (2018). Prevalence of Anal Incontinence and Constipation in Female Patients with Urinary Incontinence. Journal of Urological Surgery, 5(1), 21–24. https://doi.org/10.4274/jus.1732
Storey, J. E. (2020). Risk factors for elder abuse and neglect: A review of the literature. In Aggression and Violent Behavior (Vol. 50, p. 101339). Elsevier Ltd. https://doi.org/10.1016/j.avb.2019.101339
Suryadinata, R. V., Wirjatmadi, B., Adriani, M., & Lorensia, A. (2020). Effect of age and weight on physical activity. Journal of Public Health Research, 9(2), 187–190. https://doi.org/10.4081/jphr.2020.1840
Swenson, C. W., Masteling, M., DeLancey, J. O., Nandikanti, L., Schmidt, P., & Chen, L. (2020). Aging effects on pelvic floor support: a pilot study comparing young versus older nulliparous women. International Urogynecology Journal, 31(3), 535–543. https://doi.org/10.1007/s00192-019-04063-z
Tomasi, A. V. R., Dos Santos, S. M. A., Honório, G. J. D. S., & Locks, M. O. H. (2017). Incontinência urinária em idosas: Práticas assistenciais e proposta de cuidado em âmbito da atenção primária de saúde. Texto e Contexto Enfermagem, 26(2). https://doi.org/10.1590/0104-07072017006800015
United Nations. (2019). World Population Ageing – Highlights. In Department of Economic and Social Affairs – Population Division.
VU, H. T. (2018). Association between Diabetes Mellitus and Urinary Incontinence in Elderly Patients. Diabetes, 67(Supplement 1), 1481-P. https://doi.org/10.2337/db18-1481-p
