Selected Disease
Cockayne syndrome; also known as Neill-Dingwall syndrome. It was named after Edward Alfred Cockayne, an English Physician who first described it (1880-1956). The second name is associated with two women (Mary M. Dingwall and Catherine A. Neil) who also described it in two patients and asserted it was the same as the one described by Edward.
Mutation
Cockayne syndrome is caused by mutations in the ERCC8 or the ERCC6 genes. These genes hold instructions for making proteins that are responsible for the repair of damaged DNA. DNA can be damaged by chemicals, radiation, ultraviolet rays, and free radicals.
Symptoms
The disorder manifests in three types Cockayne Type I, Cockayne Type II, and Cockayne Type III. For Type I, babies appear normal at birth, but symptoms develop with the first and second years. Type II is the most severe while Type II is similar to Type I but milder.
The disorder is characterized by failure to gain weight, an abnormally small head (microcephaly) , short stature, severe teeth cavities, delayed growth and development, skin issues (such as lack of sweating), eye anomalies, and prematurely aged appearance (progeria). The signs and symptoms of this rare disorder are usually visible from infancy and can get worse with time (Lehmann, 2003). The most affected individuals have a high degree of photosensitivity and may experience sunburns or blisters upon short exposure to sunlight.
DNA Replication and Repair
The diagram below illustrates the normal nucleotide excision repair (NER) pathway. A NER is a vital excision mechanism that ejects DNA damage. The two subpathways of NER, transcription-coupled repair (TC-NER/TCR) and global genome repair (GG-NER/GGR) differ only in the initial damage recognition step. GGR utilizes the XPC-XPE protein complexes, while in TCR the NER proteins are recruited by the stalled RNA polymerase in mutual aid with ERCC8 and ERCC6. After recognition, the lesion is demarked by the binding of the transcription factor IIH (TFIIH) complex, RPA, and XPA. The TFIIH complex helixase function unwinds the DNA and generates an open stretch around the lesion, at which point XPF-ERCC1 and XPG endonucleases make incisions at the 5’ and 3’ ends, respectively to release a 25-29 oligomer (Koch et al., 2014). The created gap is then filled by polymerases assisted by PCNA and RCF to finally ligate the strand.
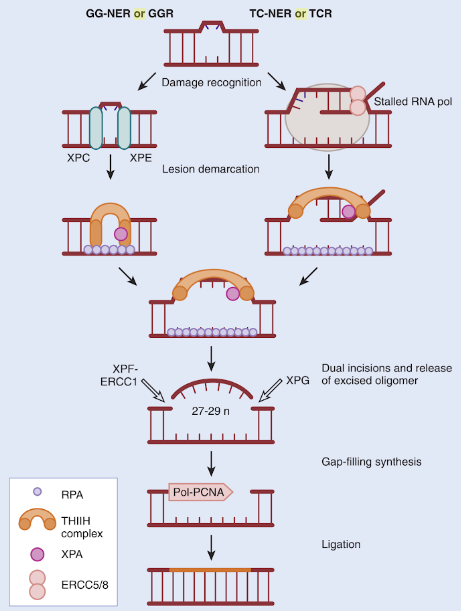
Figure 1: DNA damage and Repair (Clinical Gate, 2015)
In contrast to cells with normal repair ability, ERCC8 or the ERCC6 deficient cells are unable to perform DNA transcription coupled nucleotide excision repair (TC-NER).
References
Clinical Gate. (2015). Dna Damage and Repair. [online] Available at: https://clinicalgate.com/dna-damage-and-repair/ [Accessed 15 Jul. 2018].
Koch, S., Garcia Gonzalez, O., Assfalg, R., Schelling, A., Schäfer, P., Scharffetter-Kochanek, K., & Iben, S. (2014). Cockayne syndrome protein A is a transcription factor of RNA polymerase I and stimulates ribosomal biogenesis and growth. Cell Cycle, 13(13), 2029-2037.
Lehmann, A. R. (2003). DNA repair-deficient diseases, xeroderma pigmentosum, Cockayne syndrome and trichothiodystrophy. Biochimie, 85(11), 1101-1111.
